
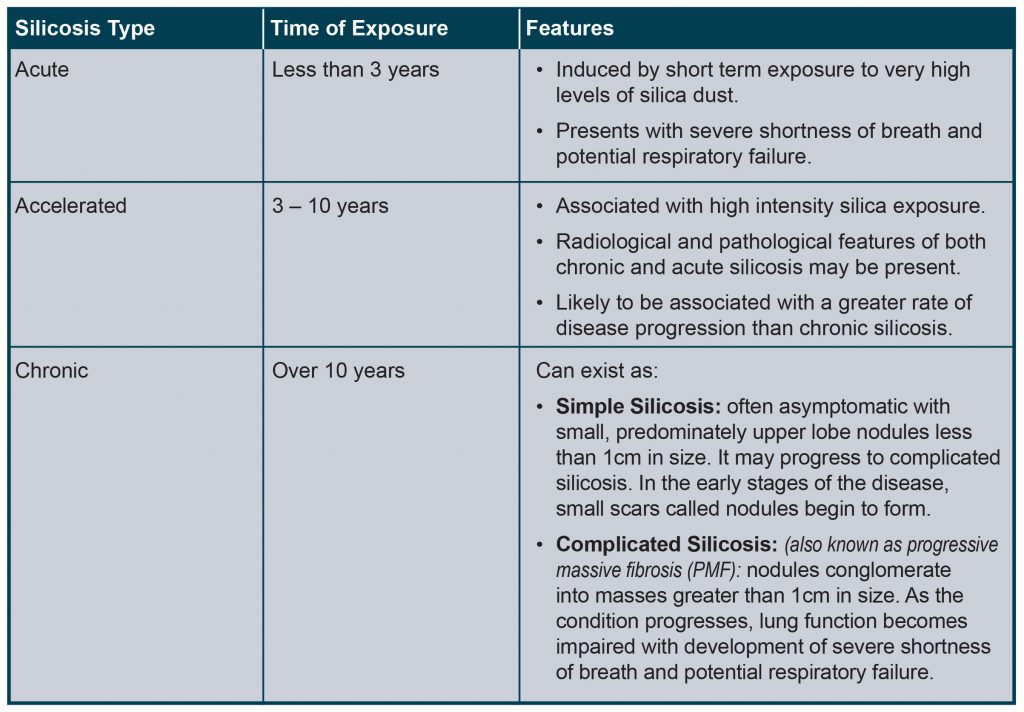
Silicosis
Silicosis is a dust related lung disease that occurs when the human body is unable to break-down or remove certain types of dust once it has entered deep into the lungs. Silicosis is a progressive fibrotic process following inflammatory damage caused by silica exposure and the body’s response. The fibrotic nodules initially form around the respiratory bronchioles in the peripheral lung. Over time, lung capacity decreases, and people with silicosis may need support with oxygen and other devices to help them breathe.
RCS Exposure in the Workplace – the Science
Dust “fractions” – size matters! To understand the potential risks to workers more clearly, it is necessary to explain what makes up the dust created by industrial processes. Not all crystalline silica dust particles are the same size. Like chipping ice from a block, processes like drilling and crushing cause different sized pieces to be broken off. The smallest pieces become airborne, and form a cloud of dust. Within this cloud there are many different sizes of particle, measured by diameter in microns, symbolised by μm (millionths of meters, or thousandths of millimetres).
Different sized particles are grouped together into three ‘fractions’ – the ‘inhalable’, ‘thoracic’, and ‘respirable’. The ‘inhalable fraction’ includes all of the particles in the dust cloud, which range from 1 to 100μm in size. These are all small enough to be breathed into the nose or mouth. The ‘thoracic fraction’ includes particles ranging from 1-30μm, which are
able to penetrate into the lungs. The ‘respirable fraction’ are particles from 1-10μm in size, which are able to penetrate into the gas exchange areas of the lungs, and cause irritation. RCS is exclusively made up of the ‘respirable fraction’.
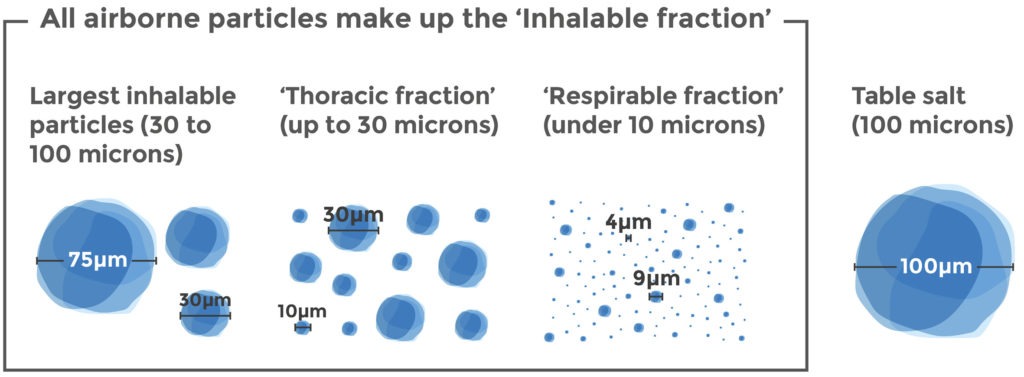
The largest inhalable particles (30 to 100 microns in diameter)
The majority of particles in a dust cloud are between 30 and 100 microns in diameter, comparatively large enough to be captured by cilia hairs in the nose and throat, and safely expelled through coughing, sneezing or blowing one’s nose. It is these 30 to 100 microns diameter particles which can most commonly be seen by the naked eye and are large enough to be picked up and carried by the wind over long distances – much in the same way that sand can be blown across a beach in windy weather.
Crystalline silica particles of this size do not stay in the body and pose no risk to health.
‘Thoracic fraction’ (up to 30 microns in diameter)
The thoracic fraction is made up of dust particles smaller than 30 microns in diameter. These particles are small enough to move past the cilia hairs in the nose and throat and may enter the sinuses and the airways of the lung. Once there, the particles sized between 10 and 30 microns are big enough to be trapped by the body’s natural defences and prevented from going further. They are then breathed out, coughed out or sneezed out.
Particles of this size do not pose a health risk, as they are dealt with by the body’s natural defences.
‘Respirable fraction’: RCS dust (under 10 microns in diameter)
The third and smallest fraction of crystalline silica particles is the respirable fraction or RCS. This fraction is small enough to penetrate the natural defences of the nose, throat and lungs, and enter the tiny vessels deep in the lungs where gas is exchanged in the breathing process.
It is in these gas exchange areas that RCS can cause irritation and inflammation. The cumulative effect of repeated high doses of RCS can cause silicosis, which in turn can increase the risk of lung cancer.
Silicosis and Lung Cancer – the Facts
For many years, it has been known that prolonged inhalation of respirable crystalline silica dust may cause a specific type of lung damage called silicosis. In fact, silicosis is often referred to as the world’s oldest known occupational disease.
Although silicosis has been recognised for centuries, our understanding of how it works and its links to lung cancer have become better understood over the past two decades. A suspicion of lung cancer occurrence among workers exposed to RCS was first proposed in the 1960s. However, confirmation of a link between prolonged silica exposure and lung cancer
was generally considered impossible until the 1980s.
In 1987, the International Agency for Research on Cancer (IARC) carcinogen for the first time, and in 1997 concluded on the basis of a literature review that inhaled RCS from occupational sources is carcinogenic to humans. In 2012, IARC confirmed its conclusions as: “Crystalline silica in the form of quartz or cristobalite dust is carcinogenic to humans”.
It is now accepted in medical science that prolonged and intense RCS exposure can cause lung cancer. To understand more about the risks to those working in industrial environments, a hazard assessment of the health effects of RCS was commissioned in 2009, run by a team of scientific experts.
The assessment concluded that:
• Silicosis is the primary health effect of direct, long-term RCS exposure.
• Any potential cancer risk due to RCS exposure is limited to lung cancer.
• Any lung cancer excess risk is demonstrated only under high occupational exposures to RCS.
• Any cancer effect is indirect/secondary to lung inflammation.
This means that silicosis is the primary risk to those working in industrial environments and that cases of lung cancer caused by RCS exposure are caused first by lung inflammation. This means that minimising the risks of silicosis in those working in industrial environments will also minimise or even eradicate the risk of lung cancer from RCS exposure. This view was validated by the European Scientific Committee for Exposure Limit Values (SCOEL), who in a 2003 report concluded that:
Preventing the onset of silicosis will also reduce the cancer risk.
This understanding has helped policy makers and regulators implement regulations to protect workers’ health, and the industries concerned to adopt measures to protect workers from the risks of RCS.
